
Injectable Polynucleotide Therapy for Genitourinary Syndrome of Menopause
Genitourinary Syndrome of Menopause (GSM) is a common yet often under-recognised condition that affects a significant proportion of postmenopausal women. Despite its high prevalence, many patients remain untreated or under-treated, particularly when first-line options fail to provide relief. In this article, I share the case of a 58-year-old patient whose GSM symptoms persisted despite systemic HRT and local vaginal oestrogen, and who responded well to a series of injectable biostimulation treatments with NewGyn®, a polynucleotide-based therapy.
![]()
Understanding GSM
GSM encompasses a wide spectrum of symptoms resulting from oestrogen deficiency, including vaginal dryness, burning, irritation, itching, urinary discomfort, and dyspareunia (painful intercourse).1 Unlike vasomotor symptoms, which tend to subside over time, GSM symptoms persist or worsen without intervention.2 These symptoms can significantly affect quality of life, sleep, sexual health, and emotional wellbeing.3
While topical oestrogen remains a cornerstone of management, it’s not always effective, and not always appropriate for every patient.4 For those who are either contraindicated for hormonal treatment or unresponsive to it, we must look beyond the conventional.
Case overview
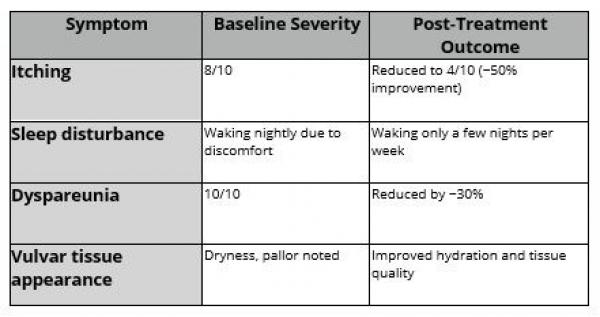
This patient was 58 years old and already established on HRT. Despite systemic support, she continued to struggle with:
- Severe itching: rated 8/10, affecting daily functioning
- Sleep disturbances: waking nightly due to discomfort
- Dyspareunia: rated 10/10, causing significant distress
She had also trialled local vaginal oestrogen, but reported no significant improvement. On examination, findings were in keeping with GSM symptoms; with dryness, areas of pallor noted with no underlying anatomical changes to the vulval anatomy.
Treatment choice and protocol
We discussed injectable biostimulation with NewGyn®, and the patient was fully informed and consented to treatment.
NewGyn® is an injectable biostimulatory formulation composed of highly purified polynucleotides (Polynucleotides HPT®), hyaluronic acid, and mannitol in an isotonic gel. The polynucleotides – derived from salmon trout DNA using advanced purification and sterilisation methods – act by stimulating fibroblast proliferation, enhancing collagen and elastin synthesis, promoting hydration, and exerting potent antioxidant and anti-inflammatory effects.5-7 The inclusion of hyaluronic acid contributes additional support for hydration and tissue elasticity, while mannitol helps protect the hyaluronic acid from enzymatic and oxidative degradation, extending the product’s bioactivity.5,8
We proceeded with a course of five NewGyn® sessions, scheduled three weeks apart.
Each session followed a standard protocol:
- Topical anaesthetic (Emla cream) applied for 25 minutes
- 2ml of NewGyn® injected subdermally across the vulvar region using a 30G needle
- Treatment duration: Approximately 10 minutes
The treatment was well tolerated. She reported a mild burning sensation after the first session (consistent with polynucleotide-based therapies), but found all subsequent sessions completely pain-free. She was pleasantly surprised by how comfortable the procedure was overall.
Clinical outcome
We followed up one month after the final (fifth) treatment. Improvements were already becoming evident:
- Itching reduced by approximately 50% (now rated 4/10)
- Sleep disturbances also decreased in both frequency and intensity, with the patient waking just a few nights per week
- Dyspareunia reduced by around 30%, an encouraging sign so soon after treatment
In addition, the appearance of the vulva improved in terms of hydration and tissue quality – not our primary aim, but a valuable secondary benefit that may help prime the tissue for any future aesthetic or regenerative procedures.
Given the severity of her symptoms, we discussed the importance of maintenance. I typically recommend reassessment and repeat treatment every six to eight months, particularly for patients who see meaningful improvements. A full five-session course takes approximately four months to complete, so two cycles per year can be a practical and effective ongoing strategy.
One of the advantages of NewGyn® is its flexibility – the treatment can be tailored to the patient’s baseline symptoms, response, and personal goals.
Challenges and considerations in introducing intimate health injectable treatments
In truth, one of the ongoing challenges with treatments like this is how to communicate their value to patients – especially in traditional gynaecological settings, where injectable regenerative options are still unfamiliar. Understandably, patients may feel hesitant when they hear the word “injection” in the context of intimate health.
That’s why patient education, reassurance, and rapport are crucial. I always emphasise that the procedure will not proceed unless the patient is fully comfortable. In practice, the vast majority tolerate it extremely well with just topical anaesthetic. We have stronger anaesthetic creams or ice on standby for more sensitive patients, but we rarely need them.
My key recommendations for those introducing NewGyn® or similar injectable therapies into their practice are:
- Choose the right patient – someone engaged, motivated, and open to regenerative options, with clinical features that support suitability for biostimulatory therapy (e.g. mild to moderate vulvovaginal atrophy, hormonal contraindications, or preference for non-hormonal treatment)
- Invest time in informed consent and explanation – cover expectations, sensations, and outcomes
- Ensure comfort – use effective topical anaesthesia and reassure the patient throughout
- Be flexible – tailor the protocol based on symptoms, severity, and patient response
It’s also important to note that before offering intimate health treatments, you must be confident in recognising conditions that can occur in the vulva (e.g. other vulval dermatoses or cancer) and have appropriate referral pathways in place if concerns arise.

Key reflections
NewGyn® has been a valuable addition to my practice for managing GSM in patients who do not respond to or are unsuitable for hormonal therapies. In this case, the patient experienced meaningful relief from symptoms that had previously caused distress in multiple domains of her life.
With regenerative treatments like this, we’re not just improving local tissue health – we’re restoring confidence, intimacy, and overall wellbeing. As awareness grows and conversations around intimate health become more open, I believe treatments like NewGyn® will increasingly form part of mainstream care.
References
- Portman DJ, Gass ML; Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and The North American Menopause Society. Menopause. 2014 Oct;21(10):1063–1068.
- Faubion SS, Larkin LC, Stuenkel CA, et al. Management of genitourinary syndrome of menopause in women with or at high risk for breast cancer: consensus recommendations from The North American Menopause Society. Menopause. 2018 Apr;25(4):596–608.
- Pastor Z, Hlavackova M, Uzel R. Impact of genitourinary syndrome of menopause on quality of life. Int J Environ Res Public Health. 2022;19(13):7617.
- MacBride MB, Rhodes DJ, Shuster LT. Vulvovaginal atrophy. Mayo Clinic Proceedings. 2010 Jan;85(1):87–94.
- Di Pietro S, Russo R, Gennari R, et al. Vulvar rejuvenation with Polynucleotides HPT and benefits on postmenopausal sexual life disruption.Obstetrics & Gynecology Research. 2022;6(3):1–7.
- Palmieri B, Rottigni V, Iannitti T. Preliminary study of polynucleotide skin applications in aesthetic medicine. Dermatol Ther. 2014 May-Jun;27(3):143–147.Palmieri B, Capone S, Capone G, et al. Polynucleotides and hyaluronic acid: a new dermal biorevitalization treatment. J Cosmet Dermatol. 2019 Jun;18(3):896–901.
- Casabona F. Use of polynucleotides associated with hyaluronic acid for vulvovaginal rejuvenation in menopause: a pilot study. Eur Rev Med Pharmacol Sci. 2022 Apr;26(7):2603–2610.